
Qifang Liu, MD, PHD; Long Yang *, MD, PHD
Department of Cardiology,Guizhou Provincial People's Hospital, 83 Zhongshan East Street,Guiyang, China.
*Corresponding author: Long Yang, Department of Cardiology,Guizhou Provincial People's Hospital, 83 ZhongShan East Street,Guiyang, China.
Received Date: September 09, 2023
Accepted Date: October 14, 2023
Published Date: November 30, 2023
Citation: Liu Q, Yang L. (2023) “-R interval monitoring for the Differential Diagnosis of Wide Complex Tachycardia.” J Clinical Cardiology Interventions, 3(2); DOI: http;//doi.org/10.2023/07.1036.
Copyright: © 2023 Long Yang. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
A previously asymptomatic 46-year-old man presented to the emergency department with sudden-onset palpitations that persisted for 90 minutes. The patient had a history of hypertension for 5 years. The blood pressure was 102/65 mmHg, heart rate (HR) was 216 bpm. The physical examination results were unremarkable, and the results of laboratory tests were normal.
Introduction
A previously asymptomatic 46-year-old man presented to the emergency department with sudden-onset palpitations that persisted for 90 minutes. The patient had a history of hypertension for 5 years. The blood pressure was 102/65 mmHg, heart rate (HR) was 216 bpm. The physical examination results were unremarkable, and the results of laboratory tests were normal. The electrocardiogram (ECG) on admission showed a wide QRS tachycardia at a rate of 216 beats per minute. There was a left bundle branch block morphology with normal axis (Figure 1).
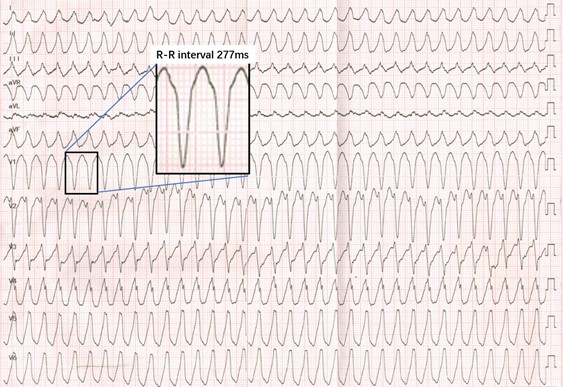
Figure 1: The admission ECG showed a wide QRS tachycardia at a rate of 216 bpm (277ms).
A repeated ECG about 12 minutes later showed a narrow QRS tachycardia triggering a sustained wide complex tachyc(Figure 2).
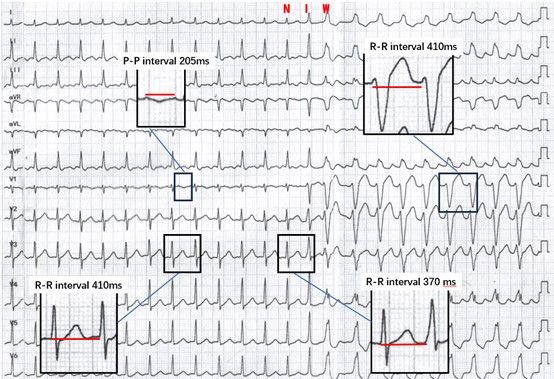
Figure 2: Cycle length measurements in atrium with the P-P (205ms) and ventricle with R-R intervals (410ms) during tachycardia. The preceding narrow complex beat and the pre-excited beat with R-R interval (370 ms). I intermediate beat; N narrow complex beat; W wide complex beat.
Questions: What is the most likely diagnosis for the first ECG (figure 1)?
Interpretation
The ECG on presentation showed a regular wide QRS complex tachycardia with QRS duration of more than 160 milliseconds and a rate of 216 beats per minute (R–R intervals 277ms). The differential diagnosis for this wide complex tachycardia includes supraventricular tachycardia with aberrancy, pre-excited supraventricular tachycardia, antidromic atrioventricular reciprocating tachycardia, and ventricular tachycardia (VT). However, the diagnosis might be confirmed on the second ECG (Figure 2) recorded on the same patient in minutes, which demonstrated a narrow-wide QRS complex tachycardia with a rate of 140 beats per minute. Flutter with 2:1 atrioventricular conduction was visualized at a P-P interval of 205ms, suggesting the presence of an atrial tachycardia or atrial flutter. The R–R intervals (410ms) of the narrow QRS tachycardia were equal to the R–R intervals (410ms) of the wide complex tachycardia. The identical rate supported the diagnosis of supraventricular tachycardia with atrial participation for wide complex tachycardia. On close inspection of the second ECG,the R–R intervals (370ms) between the preceding supraventricular beat and the fusion beat were shorter than the R–R intervals (410ms) of the tachycardia. The diagnosis of pre-excited atrial flutter was confirmed, and the apparent delta waves were seen in leads V2 and V3 even though normal P-R interval.
As for the first ECG,the R–R interval was 277ms and there was identical wide QRS morphology to the second ECG. The rate of both ECG is not the same and excluded the possibility of the pre-excited atrial flutter with 2:1 or 1:1 atrioventricular conduction. The differential diagnosis for this wide complex tachycardia includes a new pre-excited atrial tachycardia or antidromic atrioventricular reciprocating tachycardia for the same QRS morphology. The electrophysiology study demonstrated atrioventricular accessory pathway with anterograde decremental conduction property (Mahaim) [1]. The programmed atrial stimulation was positive for the inducibility of atrial flutter with 2:1 atrioventricular conduction through accessory pathway and antidromic atrioventricular reciprocating tachycardia. The radiofrequency ablation of the right free-wall accessory pathway was successfully performed, and the patient was discharged with antihypertensive drug therapy.
Discussion
This case illustrates the importance of closely measuring R–R intervals and observing the QRS morphology before determining the diagnosis for a wide complex tachycardia. First, progressive manifestation of pre-excitation should be differentiated from progressive aberrancy that may be observed at the onset of narrow-wide complex tachycardia. Progressive aberrancy can occur at the onset of tachycardia owing to differential delays in the right and left bundle branches [2]. The PR interval preceding a QRS complex that exhibits an intermediate degree of aberrancy is longer than the PR interval of a sinus beat. As a result, the R-R interval between the preceding supraventricular beat and the beat with aberrancy tends to be longer than the R-R intervals of the preceding supraventricular tachycardia [3]. For progressive manifestation of pre-excitation, the R-R interval between the preceding supraventricular beat and the pre-excited beat tends to be shorter than the R-R intervals of the preceding narrow complex tachycardia. Second,the R-R interval of wide and narrow complex tachycardias is about the same, and they are recorded within a close time span of each other. This suggests a unifying diagnosis of supraventricular tachycardia based on the principle of Occam’s razor. Third, the identical morphology wide complex tachycardia with different R-R interval usually suggest the similar tachycardia mechanisms (supraventricular or ventricular). In this case, the presence of atrial flutter does not preclude the spontaneous transition from one supraventricular tachycardia into another. In all, extended R-R interval and QRS morphology monitoring often provide critical information that can facilitate the diagnosis of WCT.
Conflicts of Interest: There are no conflicts of interest to declare.

Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org